When we talk about arthritis we are actually referring to a group of inflammatory rheumatic diseases, among which the main ones are rheumatoid arthritis, psoriatic arthritis, Reiter's syndrome and reactive arthritis, ankylosing spondylitis, arthritis associated with chronic enteropathies and acute articular rheumatism. We will talk about rheumatoid arthritis here (AR).
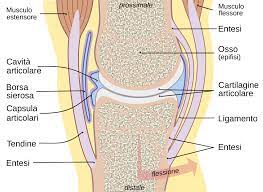
Rheumatoid arthritis (AR) it is a chronic disease that affects the diarthrodial joints, as in the case of osteoarthritis, but through a different pathological process. Unlike osteoarthritis then, RA does not only manifest itself at the level of the joints but can also involve other body structures.
At the epidemiological level AR has a prevalence between 0,3% e 2% of the population with an incidence between 2 e 4 new cases on 10.000 inhabitants each year. It occurs most frequently among the 40 e i 60 years, although it can occur in any age group, and the female/male ratio is 4 a 1.
Male/female relationship 1/4
From an etiopathogenetic point of view to date the most accredited hypothesis for the onset of RA sees the interaction between a genetic predisposition and environmental factors. The contact with an antigen that would trigger the pathological process would be crucial. This appears to consist in the mode of activation of the immune system: an acute inflammatory process which would then become chronic. It seems highly probable that in the process of maintaining the pathology autoimmune mechanisms come into play that could target collagen. To date it is not clear what the antigen in question could be but it is assumed to be a infectious agent due to the fact that, at an experimental level, it has been possible to induce chronic arthritis, similar to AR in pigs, after inoculation with a gram-positive bacillus (Erysipelothrix rhusiopathiae). To corroborate this hypothesis we add the results of research relating to reactive arthritis. These, indeed, were found to be linked to the action of bacteria such as Yersinia, Salmonella, Shiglla and Chlamydia, which would trigger its occurrence (for this reason they are called "reactive").
Between bacteria and viruses, there are many possible candidates in the search for the etiological triggering agent of RA but to date no answer has yet been reached, due to the fact that no microorganism has ever been isolated in the affected joints of subjects with RA. The virus that researchers are most suspicious of is theEpstein-Barr, the infectious mononucleosis virus, because 80% of patients with RA appear to have come into contact with it.
genetic factors
Environmental factors: infectious agents such as viruses and bacteria
At the level of the joints the target of pathological process it is the synovial tissue that thickens and produces villi. In the early stages of the disease, the main symptoms are asthenia, the appearance of slight swelling in the small joints of the hands and feet which are painful to palpation. It usually starts appearing there joint stiffness: shows up in the morning (morning stiffness) e, unlike osteoarthritis, lasts one to three hours. In some cases, fever is also present, weight loss and muscle pain. In the acute phases at the level of the joints there is also redness and heat, typical signs of inflammation (celsus, famous doctor who died in 45 d.C., defined the former 4 main elements of inflammation, heat, blush, tumor and pain, to which Galen later added the fifth, la function injured. These 5 criteria are still considered valid).
Stiffness can actually appear even later in some cases while fatigue and weakness in the movement of the affected joints appear from the beginning.
Subsequently, one can intervene functional limitation due to the extension of the inflammatory process to cartilage and to the bone immediately below it, which can undergo erosion and osteoporotic phenomena, thickening of the joint capsule and increased intra-articular fluid. In some cases, ankylosis may occur. ,
Heat
Blush
Tumor
Pain
Damaged function
The distribution of the affected joints it is symmetrical at the level of several joints (polyarthritis) diartrodiali. The temporal trend sees the more peripheral articulations affected first and gradually the more central ones: polyarthritis with a symmetrical distribution with a centripetal trend and an additive character (over time, the number of joints involved increases). This last feature differentiates RA from acute articular rheumatism which, in addition to having a limited duration, is usually of the replacement type (regresses in some joints to manifest itself in others).
The inflammatory process can also affect tendons and ligaments at the level of which nodules may appear (rheumatoid nodules). Nodules are found in only a small percentage of patients (about the 15-30%). These are usually positive patients rheumatoid factor (FR), an autoantibody that is found in a certain percentage of patients with RA. Autoantibodies attack the cells of the body that produces them because it mistakenly does not recognize them as the body's own and considering them foreign acts to fight and eliminate them. They can also manifest themselves, in rare cases, at the level of internal organs such as the heart, lungs, kidneys but in most cases they do not manage to alter their function.
At the tendon level tenosynoviti, extremely frequent, they can in many cases be the presenting symptom, with pain in movement involving the affected tendons and pain to touch along their course, especially at the level of the tendons of the extensor and flexor muscles of the fingers. Trigger finger may occur.
At hand level, over time, a deviation of the fingers towards the ulnar side of the wrist may occur, due to its conformation it is called "wind gust fingers". The fingers can then take on particular conformations due to the alterations that occur at the joint level: "gooseneck" or "boutonnière" fingers( in buttonhole) depending on the inclination ratios between the phalanges. The thumb can take the Z shape.
The disease can begin acutely or insidiously and gradually.
RA tends to induce the onset or aggravation ofosteoporosis. This can occur localized at the bone ends near the joints involved in RA or it can be widespread. The latter is the consequence of the sedentary lifestyle induced by the disease and the use of corticosteroids (which are among the drugs that are used in patients with RA).
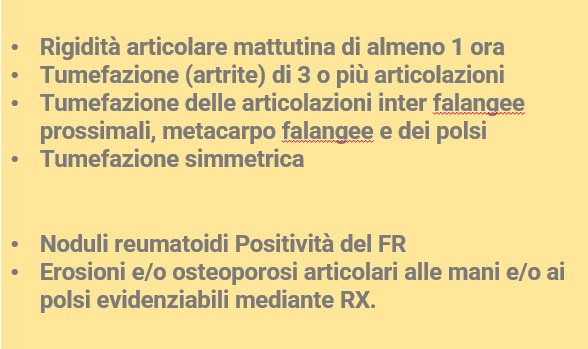
The diagnosis of RA is complex in the early stages of the disease, because its manifestations at the beginning are comparable to those of other inflammatory pathologies. The main diagnostic criteria are the presence of:
Table of criteria for classifications of rheumatoid arthritis
First four policies must persist for at least 6 weeks and othey need to be present at least 4 of the aforementioned criteria.
Monitoring of biohumoral indices such as erythrocyte sedimentation rate (VES), the C-reactive protein (PCR) and α2 globulins, (PCR) are important for the diagnosis and for monitoring the course of RA. To these tests are added those of autoantibodies, including the FR which appears to be present in the 70-75% of patients. Based on the presence or absence of RF, we speak of seropositive or seronegative RA. It should be emphasized that RF is not exclusively present in patients with RA but can also be found in healthy subjects and in subjects suffering from other pathologies. In 20-50% of patients are found to have antinuclear antibodies (ANA) which can lead to suspect the presence of concomitant pathologies such as Sjögren's syndrome or some type of connective tissue disease.
Radiography is an examination that does not provide specific findings in the initial stages of the disease but later highlights findings strongly correlated with RA such as the presence of bone erosions at the level of the areas located between the insertion of the joint capsule and the beginning of the part of bone protected by the presence of cartilage (dette aree nude o “bare areas”). The reduction of the cartilage, unlike osteoarthritis, it is of a homogeneous type and not limited to the areas that are most subjected to the load.
The medical therapy of RA aims to counteract the inflammation and painful symptoms. Then there are new categories of drugs, including biological drugs produced by genetic engineering, that have opened the door to new treatments. From the Istituto Superiore di Sanità website (https://www.issalute.it/index.php/saluteaz-saz/a/582-artrite-reumatoide#terapia) we learn that:
Rheumatoid arthritis is a disease that persists over time (chronicle), requires prolonged therapy e, in some cases, continuous. Indeed, only a few patients reach a complete recovery while most of them have to be treated for a long time.
Therapy should be started as quickly as possible, before the inflamed joints are permanently damaged.
The evolution of the disease varies from person to person. The disturbances (symptoms) may appear gradually, even over the course of several weeks or a few months.
Most sufferers go through periods characterized by disturbances (symptoms) acute alternating with periods in which the pain is almost absent.
In Italy, the number of cases of rheumatoid arthritis in the general population (prevalence) is approximately equal to 0,5% and the sick are estimated to be among the 200.000 e i 300.000.
THE REHABILITATION
Rehabilitation is very important for patients suffering from this pathology. RA is a disease that undergoes active phases and phases of remission.
If it is true that in active phases, where the inflammation is present, it should be recommended to keep the joints at rest, in the phases of remission it is essential to intervene to keep one proper joint function and prevent them from undergoing structural alterations that could otherwise degenerate into important situations such as ankylosis. The rehabilitation intervention also aims to maintain/restore the right tone level, forza, muscle mass and function necessary for the proper functioning of the joints. The muscles, indeed, in this pathology they are affected both by periods of inactivity due to the active phases of the pathology and by the side effects of cortisone (cortisone myopathy).
Correct muscular activity is necessary to protect the joints from functional overloads and incorrect movements that can contribute to altering their structure.
BIBLIOGRAPHY:
German, Silvanus, Pier Franca Gambari, and Leonardo Punzi. Rheumatic diseases. McGraw-Hill, 2007.